


Eliminating the Exit Dose
Cancer treatment is a tricky balancing act: damage as much cancer as you can without making the cure worse than the disease. After X-rays were discovered in 1895, the medical world learned that radiation could shrink tumors. But physicians soon discovered it could cause the very disease it was treating when radiologists who had tested dose strength on their arms later developed leukemia.
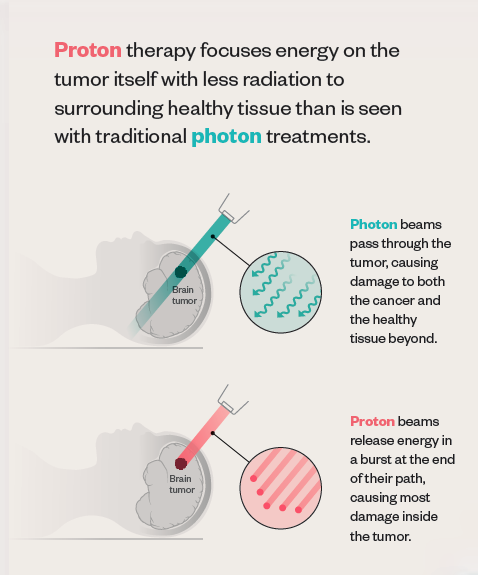 Traditional radiation uses photons, packets of energy that cause damage to all the cells they encounter along their path, with no way to control where that path ends. “After it passes through the tumor, the photon beam continues on out of the patient, depositing some ‘exit dose’ in healthy tissue,” explains Bill Salter, professor and chief of the Division of Medical Physics in the U’s School of Medicine and senior director of radiation oncology at HCI.
Traditional radiation uses photons, packets of energy that cause damage to all the cells they encounter along their path, with no way to control where that path ends. “After it passes through the tumor, the photon beam continues on out of the patient, depositing some ‘exit dose’ in healthy tissue,” explains Bill Salter, professor and chief of the Division of Medical Physics in the U’s School of Medicine and senior director of radiation oncology at HCI.
Since the turn of the 20th century, scientists have known that protons—particles inside atoms—travel a finite depth and deposit most of their energy at the end of their path, a property known as the Bragg peak. In 1946, physicist Robert Wilson published a paper proposing the use of protons in medical treatments. Because of the Bragg peak, Wilson pointed out, proton beams can travel to a tumor, deliver the dose of radiation, and then stop. In other words, no exit dose.
Proton therapy isn’t necessarily more effective at killing cancer cells. The true benefit comes from that lack of exit dose. “We use protons because that does a better job of decreasing and preventing some of the long-term toxicities of radiation,” says Poppe.
Still, most HCI patients who need radiation will continue to receive traditional photon therapy, “not because we don’t have capacity to treat them with protons, but because there’s not a significant benefit,” he notes. “Each case needs to be looked at on an individual basis.”
Life expectancy is one factor physicians consider, and young adults and children are good candidates since late effects or secondary cancers may occur several years down the road. Tumor location also factors in. Proton therapy may be recommended if the cancer is near an area of the body especially sensitive to radiation.
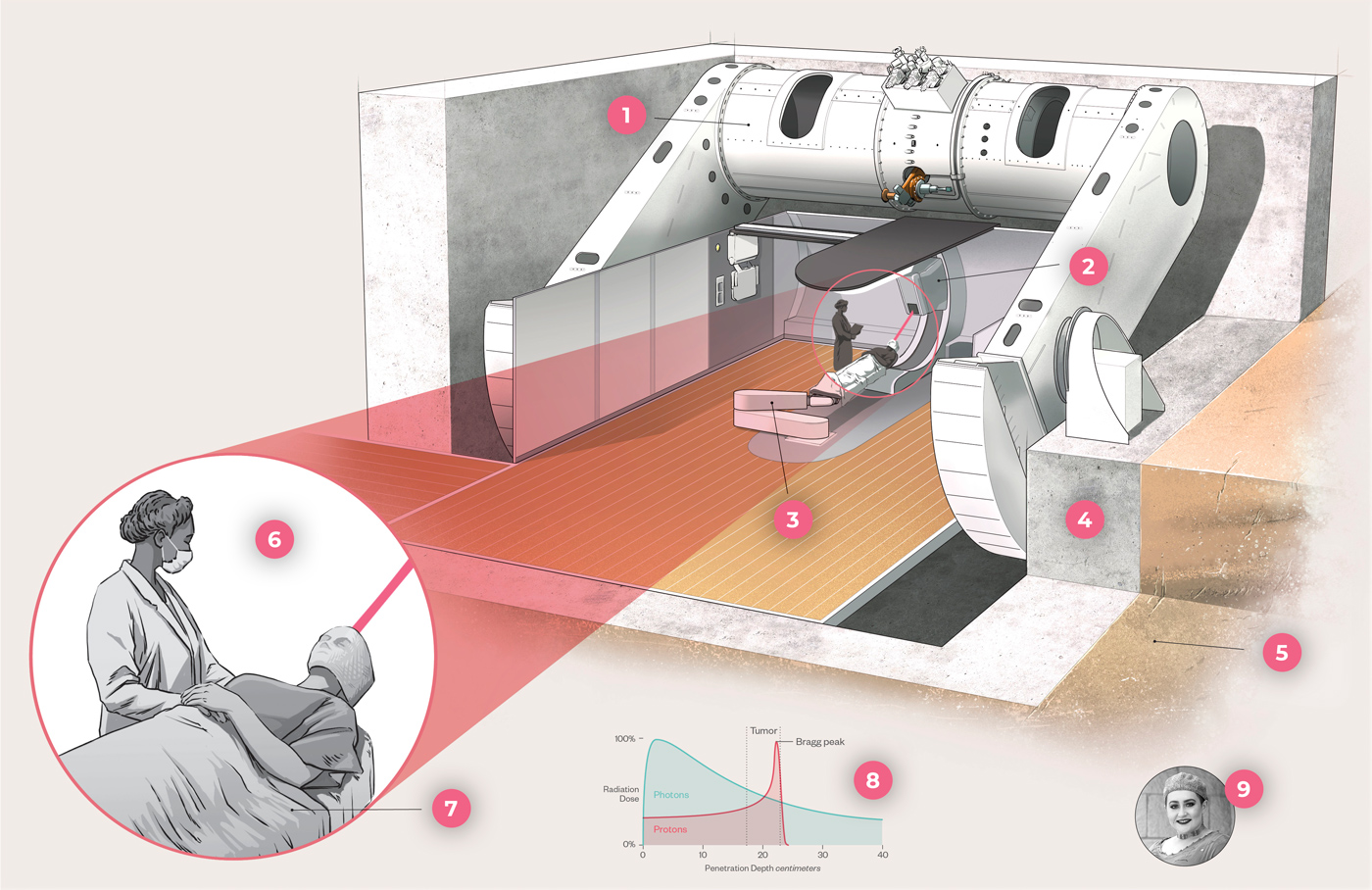
Proton therapy sessions are similar to traditional radiation. A typical course may involve daily 30-minute treatments for a period of several weeks. During treatment, a machine called a cyclotron accelerates protons to two-thirds the speed of light. A large structure called the gantry rotates the radiation beams around the patient, who typically lies in a custom-made body mold to help maintain accurate positioning as the beams enter the body at different angles.
Whether proton or photon, radiation beams don’t hurt when they enter the body. And short-term side effects—most commonly, nausea, vomiting, diarrhea, fatigue, and skin changes—are similar for both types of radiation therapy.
Moving Mountains
Though Wilson’s research was published in 1946, it wasn’t until 1990 that the first hospital-based proton therapy treatment center opened. Costly equipment and limited technology kept proton therapy on the fringes.
As technology improved and the price of equipment decreased over the decades, administering proton therapy became more feasible. But adding a proton facility is still a major undertaking. Most centers are located in big cities and are accordingly built for a large population. They typically contain four or five gantry systems, taking up the space of a football field and costing up to $250 million.
“That would not be sustainable here and would be more than we need,” says Poppe. “We were waiting for the right technology for our patient population.”
In 2012, the FDA approved the use of a compact proton therapy machine that contains a smaller, built-in cyclotron. HCI opted to install one unit, bringing the total cost of the facility to $31 million. The site contains enough room for a second machine if needed down the road. But for now, U director of radiation oncology Salter says, “We’re trying to take a reasonable bite.”
Despite having very little room to expand—HCI sits so close to the foothills that rattlesnakes and tarantulas sometimes grace the premises—leaders were committed to building the proton therapy center onsite.
“We didn’t want to split our team of experts up,” says Salter, who oversaw the building process. “We wanted those experts to be available to care for the patient, day in and day out.”
All they needed was to find an unused corner of the property to squeeze in the 7,450- square-foot building. That space was a small section between the cancer hospital and research building.
“It’s a 25-degree slope on the side of a hill, which is why it was unused,” Salter laughs. “But if we were to move a piece of that mountain, we would have a perfect spot to put this proton unit.”

In order for construction equipment to even get to the space, crews had to build a temporary road behind the HCI research building, putting in switchbacks due to the steep grade of the hill. Then came the process of digging up and moving hundreds of truckloads of mountain—not just dirt, but also rock. Blasting was not an ideal option. “We’re right here next to a research facility, which is very sensitive to vibrations,” notes Salter. The team had to come up with alternatives—a giant mechanical jackhammer to break up the large boulders or an expanding chemical material that breaks rock.
“In the end, with much persistence, the giant jackhammer did the trick,” says Salter.
While crews worked through construction hurdles, the radiation oncology team faced its own obstacle of undertaking a two-year training process. Instead of recruiting from other proton centers, leaders wanted HCI’s existing medical physicists, physicians, radiation therapy technicians, and other members of its already talented team to learn the necessary skills.
Then came COVID-19. “We had to change the original plan radically,” says Salter. “We were forced to cancel visits to outside centers and switched almost exclusively to virtual interactions.”
Through phone calls, virtual trainings from the equipment vendor, and video presentations from colleagues at other proton centers, HCI’s radiation oncology team learned the nuances of using proton therapy.
“We managed to get our entire team trained up in that environment,” Salter says. “We must be the only proton center in the country to go live during a pandemic.”
Comments
Comments are moderated, so there may be a slight delay. Those that are off-topic or deemed inappropriate may not be posted. Your email address will not be published. Required fields are marked with an asterisk (*).